Your on-line source for reliable and unbiased information about the evaluation & treatment of heart disease.
The heart is a muscular organ that pumps blood to the body at an average of 72 times per minute. Oxygen and nutrients serve as a fuel supply to the pump and are carried to heart in the form of blood that flows through the coronary arteries. Thus, the coronary arteries serve as fuel pipe lines to the heart muscle.
The three major coronary arteries (Left Anterior Descending (LAD), Circumflex (Circ) and Right Coronary Artery (RCA)) and their respective branches each supply a designated portion of the heart, as follows: The LAD supplies blood to the front (anterior) portion of the heart and the septum (muscle partition that separates the Left Ventricle (LV) and Right Ventricle (RV)). The Circ supplies the back (posterior) portion of the LV. The RCA supplies the bottom (inferior) portion of the ventricle and also the RV in 90% of cases. In the other 10%, the Circ sends a branch to the inferior wall of the LV.
Coronary arteries have muscle fibers within their walls. By contracting the muscle, the artery can reduce blood flow; relaxing the muscle increases flow. In this way, the coronary arteries can regulate blood flow to different portions of the heart. Occasionally, the muscle within a coronary artery may go into spasm and markedly reduce blood flow to the heart muscle. This condition is known as coronary spasm. Typically, the chest discomfort of coronary artery spasm occurs at rest, and usually during the early morning hours. When the spasm is relieved (spontaneously or with the use of medications), the blood vessel goes back to its normal appearance and function. A temporary decrease in blood supply can cause chest discomfort while a persistent decrease can result in permanent muscle damage or a heart attack.
![]()
Atherosclerosis is by far the commonest cause of coronary artery blockage. Unlike coronary spasm which creates a temporary blockage, atherosclerosis results in a fixed blockage. Occasionally, atherosclerosis may be accompanied by coronary spasm. The diagrams below show the various stages of progression of atherosclerosis and development of coronary artery blockages. The round picture on the left of each illustration is a cross-sectional view of the coronary artery, while the picture on the right is a longitudinal section at the same level.
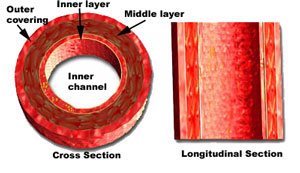
The inner lining of the normal coronary artery is smooth and free of blockages or obstructions.
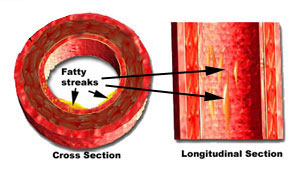
However, as we get older, lipids or fatty substances (cholesterol and triglycerides) are deposited as fatty streaks. The streaks are only minimally raised and thus do not produce any obstruction or symptoms.
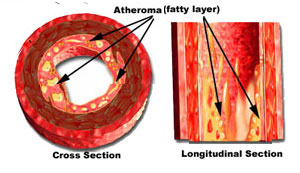
Patients with one or more risk factors for CAD are susceptible to the increased buildup of fatty layers, known as atheroma (pronounced athe-a-roma). This buildup of material begins to encroach upon the inner channel and starts to interfere with the free flow of blood through the coronary artery.
![]()
Major risk factors for developing CAD include:
- Hyperlipidemia (high cholesterol level, particularly the "bad" component known as Low-Density Lipoprotein (LDL))
- High blood pressure
- Diabetes
- Cigarette smoking
- Strong family history of CAD
- Male gender, obesity, age above 50 years, lack of exercise, stress and tension can also predispose to the development of atherosclerosis
The deposit of atheroma within the inner lining of arteries is called atherosclerosis (pronounced ath-row-sklee-rosis). It is estimated that 1/3 of adult Americans develop some form of CAD.
Significant atherosclerosis may be confined to the coronary arteries or may be associated with blockages within the arteries of the neck and those supplying blood to the lower limbs (legs)
As atherosclerosis progresses, fibers begin to grow into and around the fatty layers of atheroma, causing the blockage to harden and turn into a plaque (pronounced plak). The enlarging plaque (above) increases the encroachment into the inner channel of the coronary artery. When the channel is reduced by more than 50% (of the diameter) the artery may become obstructed enough to decrease blood flow to the heart muscle during times of increased need (exercise, emotional stress, etc.). During such times, the blood pressure and heart rate are both elevated and increase the need of oxygen and nutrients by the heart muscle.
The imbalance between the supply and demand of oxygen can cause chest discomfort (tightness, fullness, heaviness or pain) in the center of the chest and/or over the left breast). This is known as angina (pronounced an-ji-na) or angina pectoris. When the coronary artery blockage is severe enough to completely cut off the supply of oxygen and nutrients to the heart muscle, a heart attack can result. However, atherosclerosis may maintain a stable pattern for several years or even decades if the plaques grow slowly or remain relatively stationary. These patients may not notice worsening of angina during the time of stability and are said to have stable angina.
![]()
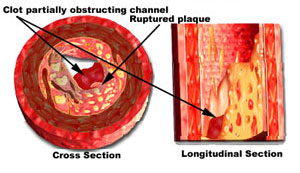
In other cases, plaques within the inner lining of the coronary artery may develop a slight crack or rupture. Note that the rupture involves only the surface and does not go through the wall of the artery. It is similar to a superficial crack on the plaster of a swimming pool lining, and blood does not escape out of the artery. Plaque rupture stimulates the production of blood clots that tries to seal off the superficial crack. The clot also gets into the crack and causes it to rise and further obstruct the channel of the artery. The sudden increase in the obstruction caused by the raised ruptured plaque and associated clot can transform a mild blockage into a critical one within a matter of hours (above). The decrease in blood flow to the heart muscle is severely reduced and the patient begins to have severe and prolonged chest pain that occurs at rest and may even awaken him or her from a sound sleep. This is known as unstable angina. If the clot does not fully close off the channel of the artery (as in the example above) enough blood flow is maintained to the heart muscle, and a heart attack may not develop if appropriate and prompt treatment is employed.
![]()
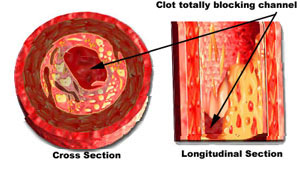
However, the clot may continue to grow in many cases. This can completely fill the open channel of the artery (above) and cut off blood flow to the part of the heart muscle that it supplies. Without oxygen and nutrients, the patient suffers from a heart attack and the involved heart muscle can get permanently damaged. The good news is that there are several forms of treatment that can get rid of the blood clot and restore flow across the artery. However, this can only be employed if the patient is rushed to the emergency room of the nearest hospital. Every minute counts in salvaging heart muscle.

Coronary artery blockages and heart attacks may also be seen in patients who use "Crack" cocaine. This is becoming one of the commonest cause of heart attacks in young adults who are treated in emergency rooms in the USA.
©1999-2017, 20XXA.S.M. Systems, Inc. All Rights Reserved, including design and all graphic contents & animations